

Danger
 The first step generally describes the initial moments when a first aider realises something is wrong – when they come across a person lying on the ground, or see them suddenly collapse for no obvious reason.
The first step generally describes the initial moments when a first aider realises something is wrong – when they come across a person lying on the ground, or see them suddenly collapse for no obvious reason.
It reminds first responders that the first thing to do is check for ongoing danger. Although our instinct may be to rush to the aid of someone who’s sick or hurt, it’s important to be cautious. You need to check if there’s an obvious cause for the person’s condition or anything that might cause other injury. Rushing in to help when there’s a venomous snake, exposed electrical wires, or fast-moving traffic nearby could mean you just end up as a casualty yourself.
If you identify danger in the area, you need to remove or control the danger. In some cases, this might involve making changes in the environment – such as switching off electricity or parking your car on the road with hazard lights on. In other cases, it may require moving the casualty. While this isn’t recommended, sometimes it’s unavoidable – performing first aid on someone lying in the middle of a busy expressway is a far bigger risk than moving them.
In some cases, the danger might mean you can’t safely approach. Trying to kill or chase away an angry snake to get to the person they’ve bitten is likely to make the situation far worse. In such cases, you need to keep your distance and call for help.
Once you’ve checked the area and found it to be safe, you can approach the person.
Response
 Once you’re able to reach the person, the first thing to check is whether they can respond to someone’s voice or touch – whether they’re awake and alert.
Once you’re able to reach the person, the first thing to check is whether they can respond to someone’s voice or touch – whether they’re awake and alert.
Start with simple questions or requests, speaking in a clear voice. Another common acronym used specifically for this step is COWS – which stands for “Can you hear me?”, “Open your eyes”, “What is your name?”, and “Squeeze my hand, then release it”. Each of these should be spoken to the person in a clear, calm voice to see if they respond. For the last question, you should place your hand in theirs, allowing them to squeeze it if they can.
If the person doesn’t respond to spoken questions, you should try firmly grasping and squeezing their shoulders to see if they respond – making sure that you don’t grasp too hard. When touching the person for any reason, you should make sure you’re not aggravating any existing injuries – or causing any other harm.
If the person doesn’t respond, or shows only a minor response (such as groaning without opening their eyes), you should regard them as unconscious and progress to the next step.
Send for Help
 If the person is unresponsive, it’s time to call for medical assistance. However, in an emergency, time is also critical.
If the person is unresponsive, it’s time to call for medical assistance. However, in an emergency, time is also critical.
If other people are present, you should ask one of them to call 000 for an ambulance using the closest available phone (normally their mobile, if they have one). This allows you to continue providing aid for the person while they call for help. Once the ambulance has been called, the person can also check the nearby area for an AED unit in case it’s required.
If you are on your own, you should start by calling for help and asking anyone who responds to call an ambulance. If no one is nearby and you have a mobile phone, you can call 000 for an ambulance and place it nearby on speaker phone mode – allowing you to continue providing first aid as you call for help.
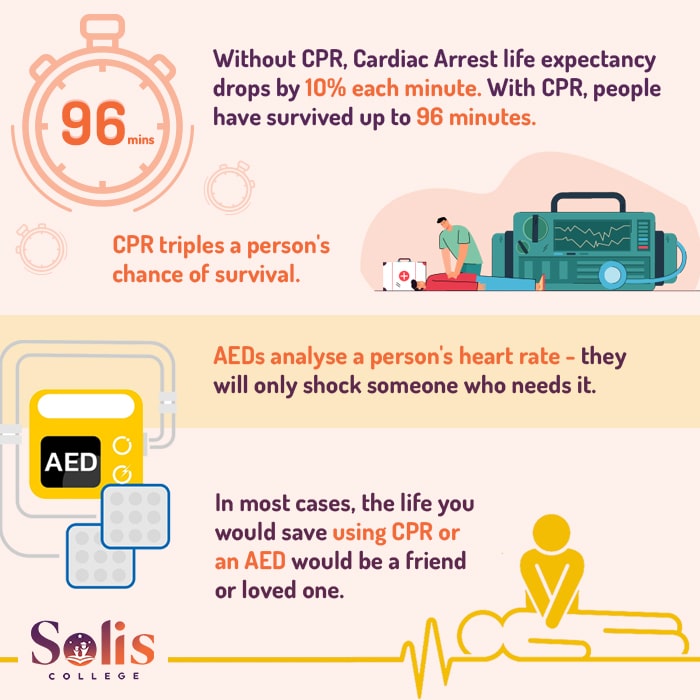
Only if there is no alternative should you leave the person to summon help or call for an ambulance – and return as quickly as possible. If the person is suffering Cardiac Arrest then every minute they go without CPR dramatically lowers their chances of survival.
Once you know medical assistance is on the way, you can move on to checking the person’s airway.
Airway
 The next priority is to ensure the person’s airway is clear and that they’re able to breathe – whether they’re currently doing so or not. It’s best not to move the person for this, but rather to check their airway is clear in the position you found them.
The next priority is to ensure the person’s airway is clear and that they’re able to breathe – whether they’re currently doing so or not. It’s best not to move the person for this, but rather to check their airway is clear in the position you found them.
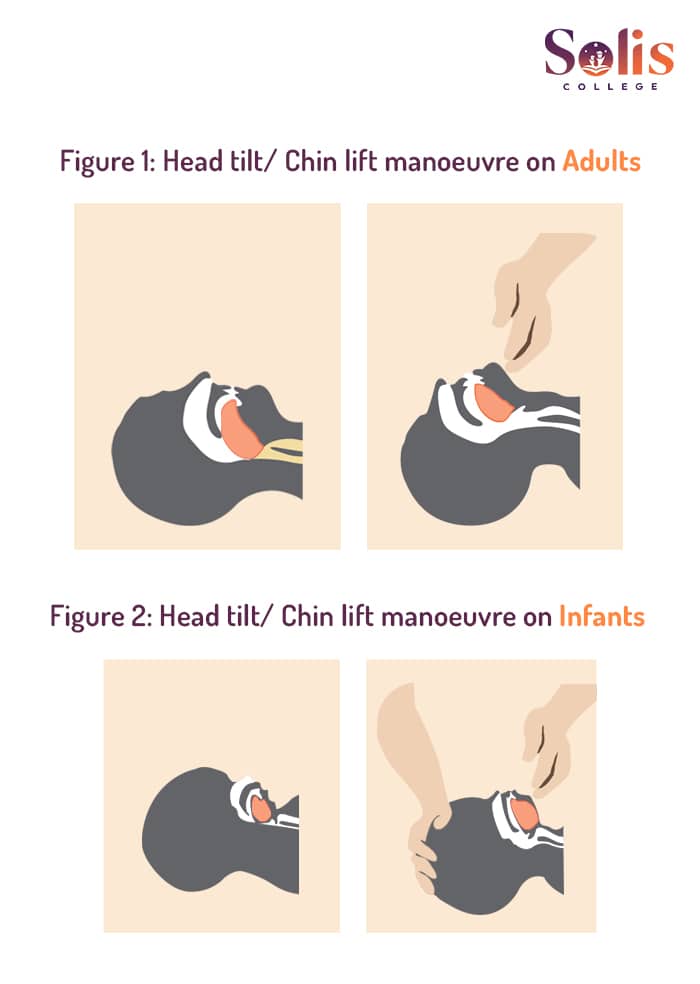
For adults and children, tilt the head back slightly while lifting the chin (as pictured) to provide the clearest possible path for breathing. For an infant, try to have their head in a neutral position – neither forward, nor backward – as their smaller windpipe can be narrowed if the head is tilted back too far.
Once the airway is correctly aligned, open the person’s mouth and look inside for signs of blockage or fluid (such as water or vomit) in the person’s windpipe. If you find anything, roll the person onto their side (if they’re not in that position already), and allow any foreign material to drain out. Any blockages that do not drain out naturally may be removed with the fingers – sweeping from one side of the mouth to the other.
Be careful when moving the person, particularly if you think they might have a neck injury. But remember that for an unconscious person, ensuring a clear airway takes priority over any other injury.
Breathing
 There are three key ways to check if someone is breathing. First, look at their chest to see if their chest is moving as they breathe – specifically, watch their lower chest and upper abdomen.
There are three key ways to check if someone is breathing. First, look at their chest to see if their chest is moving as they breathe – specifically, watch their lower chest and upper abdomen.
Note that movement in the chest may still occur if the person’s airway is blocked – which is why checking the airway first is critical.
Second, move your ear near the person’s mouth and listen for the sound of air escaping from their nose and mouth as they breathe out.
Third, if you can’t hear the air coming in and out of their lungs (perhaps due to nearby noise), see if you can feel the breath coming out.
If the person is breathing normally, this is a good sign. However, if the person is both unconscious and not breathing, they are likely suffering cardiac arrest and you should start CPR.
If someone is breathing abnormally or gasping for air while unconscious or unresponsive, you should still treat them as if they were not breathing and begin resuscitation – regular breathing is essential for life.
CPR
 A person who is unconscious and not breathing is now regarded as being in Cardiac Arrest – meaning their life is now on the line and urgent action is needed. CPR, or cardiopulmonary resuscitation is used to prolong the person’s life until help arrives
A person who is unconscious and not breathing is now regarded as being in Cardiac Arrest – meaning their life is now on the line and urgent action is needed. CPR, or cardiopulmonary resuscitation is used to prolong the person’s life until help arrives
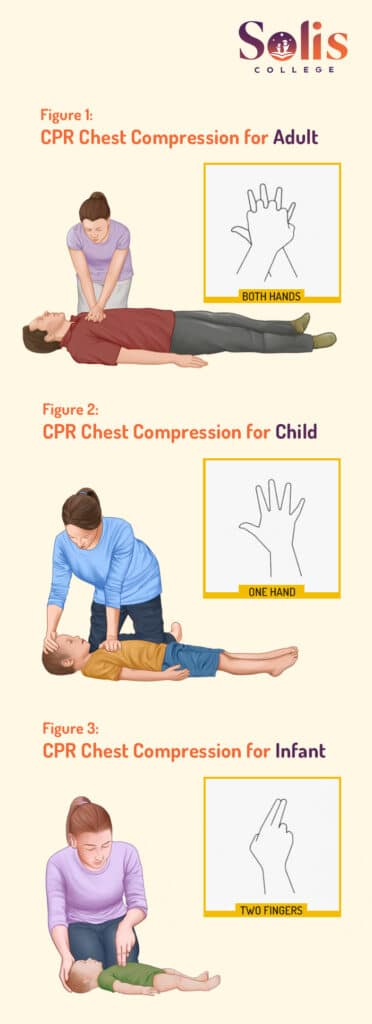
First, ensure the person is lying on their back, and get into a comfortable position beside them – you may be going for a while. Place one hand on the centre of their chest and the other hand on top of it with your fingers interlocked. Then start chest compressions, and rescue breaths – 30 compressions, 2 breaths, and then repeat.
CPR should continue until:
- The person recovers and starts breathing normally
- A medical professional arrives and takes over, or tells you to stop
- You are physically unable to continue
It’s important to note – CPR is a first aid skill, and where possible should be performed by someone with accredited first aid training. Reading a blog (no matter how useful it might be) is no substitute for being properly trained in CPR first aid and practising those skills on a proper training manikin. But we can cover a few fundamentals.
Defibrillation
 To bring someone out of cardiac arrest and prevent them from dying, the person will normally need defibrillation. Until recently, this would mean waiting for an ambulance to arrive with a portable defibrillator and then letting the paramedics connect and operate it. However, in recent years automated external defibrillators (AEDs) have become increasingly easy to use and widely available – meaning non-medical professionals can use them, and many public facilities and workplaces have AED units available for emergencies.
To bring someone out of cardiac arrest and prevent them from dying, the person will normally need defibrillation. Until recently, this would mean waiting for an ambulance to arrive with a portable defibrillator and then letting the paramedics connect and operate it. However, in recent years automated external defibrillators (AEDs) have become increasingly easy to use and widely available – meaning non-medical professionals can use them, and many public facilities and workplaces have AED units available for emergencies.
Although ideally a first aider should have been trained with an AED before using one in a medical emergency, most AEDs do come with clear printed instructions. Many modern models also have a voice function, and are designed to clearly talk the user through how to operate them.
They also automatically detect the person’s heart rhythm, detect when a shock is needed, and loudly announce when they’re about to shock and warn users to stand clear. This allows even bystanders with no training to operate one when needed – although obviously they’ll take longer than a trained user, and every second is critical when treating cardiac arrest.
Users should follow the instructions provided by the AED unit to attach the pads to the casualty. Instructions may vary from unit to unit, but some important guidelines are:
- Pads should be placed so that the person’s heart is directly between the two shock pads
- Good skin contact is needed – try to remove excess body hair and wipe away any moisture before applying a pad (but don’t take too long)
- Avoid placing a pad over an implanted medical device – or within 8cm of one (that’s about a hand’s width).
Someone should continue performing CPR while the AED is being fetched and set up, and only stop when the device is ready. Every moment without CPR lessens the person’s survival odds.
It’s worth remembering that unlike in movies and television, real defibrillators do not cause the patient to jerk dramatically when shocked. Nor do they make a loud “thunk” noise – or any sound other than warning noises made by the unit. This idea comes from television and movies, where using a defibrillator is deliberately made more dramatic and visual than in real life. So you don’t need to worry if your AED isn’t working just because the person doesn’t convulse like they do in the movies when shocked.
If the person doesn’t revive after the first shock, continue CPR until the device signals that it’s ready to shock again. Defibrillation doesn’t always work on the first attempt. Sometimes it can take hours.
What does defibrillation actually do?
The common perception of Defibrillation is that you’re using an electrical jolt to jump-start a stopped heart – like someone might jump-start a car engine with jumper leads. In reality, almost the opposite is true. Defibrillation doesn’t start the heart beating – it stops it. In fact, if someone’s heart has stopped entirely, a Defibrillator won’t help them.
In most cases, Cardiac Arrest doesn’t actually mean the person’s heart has stopped entirely. Normally, it means the person is suffering what’s called ventricular fibrillation – their heart is quivering and convulsing erratically, meaning it’s not pumping blood around the body as it would normally.
Defibrillation means giving a very controlled electric shock to stop the heart beating altogether. This then allows the heart to restart by itself a few moments later, returning to a more normal rhythm and starting the flow of blood through the body again – when it works. In a way, it’s less like jump-starting a car and more like turning a machine off and on again in the hopes that it starts correctly and fixes the problem.
If the heart has stopped beating entirely, this is referred to as asystole or cardiac flatline, and at that point, there’s normally not much anyone can do. So yes – all those movies where someone’s heart monitor goes flatline (with that long, drawn-out beep sound) and the hero jumps in to zap them back to life with defibrillator paddles? Yeah, it doesn’t really work like that. That person’s gone.